
Learning Objectives: Chest X-ray Anatomy
- This tutorial demonstrates some of the important anatomical structures visible on a chest X-ray.
- By the end of the tutorial, you will be familiar with all the important structures of the chest, which should be checked whenever you look at a chest X-ray.
Before you start, have a look at the normal chest X-ray below.

- How many anatomical structures can you see on this X-ray?
- Can you think of any important structures in the chest that are difficult to see on the X-ray?


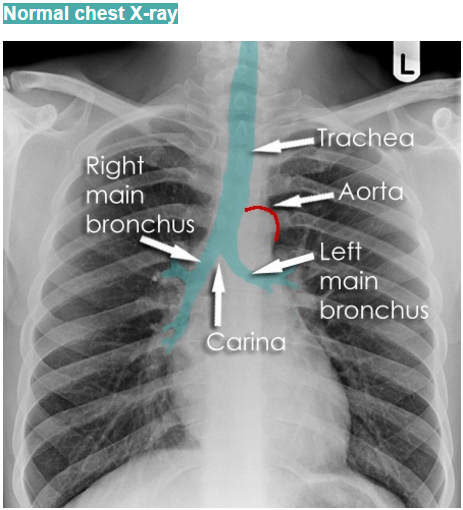
Trachea and major bronchi
- The large airways are visible on most good quality chest X-rays. They contain air and so are of lower density (blacker) than the surrounding soft tissues.
- The trachea branches at the carina, into the left and right main bronchi.
- The trachea passes to the right of the aorta and so may be slightly off midline to the right.
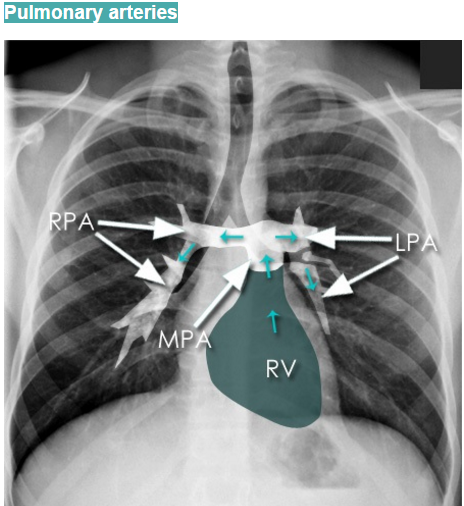
Hilar structures
Key points
- Each hilum contains major bronchi and pulmonary vessels, There are also lymph nodes on each side (not visible unless abnormal).
- The left hilum is often higher than the right, although the difference should be less than 2.5 cm.
- If a hilum is out of position, ask yourself if it has been pushed or pulled.
- As well as position – check the size and density of the hila.

Chest X-Ray Anatomy: Hilum. 
Chest X-Ray Anatomy: Hilar Structure
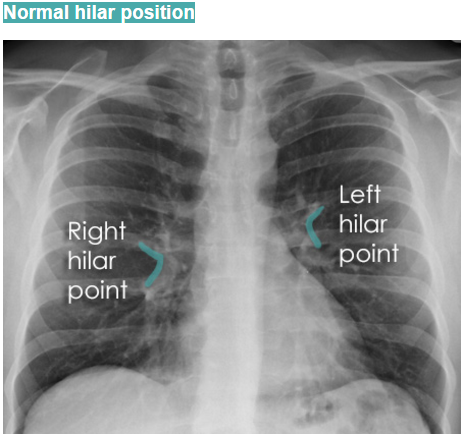
Normal Hilar Position:
- By convention, the hilar points are the angle formed by the upper lobe veins, as they cross behind the lower lobe arteries.
- Not every normal patient has a very clear hilar point on both sides, but if they are present then they can be useful in determining the position of the hila.
Lung zones

Dividing the lungs into zones allows more careful attention to be paid to each smaller area. if this is not done it easy to ignore important abnormalities.
Note that the lower zones reach below the diaphragm (dotted white line) – the lungs pass behind the dome of the diaphragm into the posterior sulcus of each hemithorax (asterisks).
Assessing the lung zones
- Each zone is compared with its opposite side paying attention to any asymmetry. These should be of equal transradiancy, and one should not be any whiter or darker than the other.
- If there is asymmetry, decide which side is abnormal. Often a dense (whiter) area is abnormal, but some diseases cause reduced density (blacker).
- You should also be aware that some diseases result in bilateral lung abnormalities, making a comparison of left with right difficult.
Pleura and pleural spaces

The pleura and pleural spaces are only clearly visible when abnormal. Some diseases, such as mesothelioma, cause pleural thickening. Other pleural diseases lead to fluid accumulation (pleural effusion) or air gathering in the pleural spaces (pneumothorax).
Assessing the pleura
- Pleural abnormalities can be subtle, so it is important to check carefully around the edge of each lung where abnormalities are seen more easily.
- Make sure you can see lung markings all the way to the edge of the chest wall. If the lung edge (visceral pleura) is visible and there is black surrounding this edge, then a pneumothorax should be suspected. This should lead to an immediate assessment of the patient’s trachea and mediastinum, both on the X-ray and, more importantly, clinically. Deviation of midline structures away from the side of a pneumothorax is evidence of a tension pneumothorax which is a medical emergency.
- Failure to diagnose a tension pneumothorax on a chest X-ray is the quickest way to fail your Radiology exam!
- Every chest X-ray should also be checked for pleural thickening, and pleural effusions.
Lung lobes and fissures
- The left lung is divided into two lobes, upper and lower by an oblique (major) fissure.
- In the right lung, there is an oblique fissure and a horizontal fissure, separating the lung into three lobes – upper, middle, and lower.
- Lateral chest X-rays are helpful in demonstrating the oblique fissures.

Left Lung: Fissure 
Rt Lung: Fissures



Horizontal fissure
- The horizontal fissure separates the right upper lobe from the right middle lobe. It can be seen (but Difficult) as a thin line running roughly horizontally from right hilum to the 6th rib in the axillary line. If it is displaced then this may be a sign of lung collapse.
Oblique fissures

The oblique fissures overlie each other on a lateral view and are not always seen in entirety. If seen at all, the lower end is usually seen most clearly, as on this X-ray.
Accessory fissures
- The most common accessory fissure you will see on a chest X-ray is an azygos fissure, This occurs in approximately 1-2% of individuals.
- The azygos vein usually runs horizontally along the right side of the mediastinum.

Costophrenic recesses and angles
- On a PA view, the costophrenic recesses are seen on each side as the costophrenic angles.
- he costophrenic angles consist of the lateral chest wall and the dome of each hemidiaphragm.
Assessing the Costophrenic Angles

- On a frontal chest X-ray, the costophrenic angles should form acute angles.
- Often the term costophrenic “blunting” is used to refer to the presence of a pleural effusion. This, however, is not always correct and costophrenic angle blunting can be related to another pleural disease, or to underlying lung disease.
- Lung hyper-expansion can also lead to blunting of the costophrenic angles. This is because the domes of the diaphragm are pushed downwards and so the angle formed is no longer acute.
Diaphragm

- he right hemidiaphragm is slightly higher than the left
- The liver is located inferior to the right hemidiaphragm
- The stomach and spleen are located inferior to the left hemidiaphragm
- Lung markings are visible below the diaphragm on both sides – most clearly through the stomach bubble
Heart size and contours
Heart size is not assessed by absolute measurement, but rather in relation to the total thoracic width, and is expressed as a ratio.
Cardiothoracic ratio (CTR) = Cardiac Width : Thoracic Width
A CTR of greater than 1:2 (50%) is considered abnormal. This, however, assumes the projection is Posterior-Anterior (PA), and that cardiac size is not exaggerated by factors such as patient rotation or an incomplete breath in.

Cardiothoracic ratio (CTR)
- Cardiac size is measured by dropping parallel lines down both sides of the heart, at the most lateral points on each side, and measuring between them.
- Thoracic width is measured by dropping parallel lines down the inner aspect of the widest points of the rib cage and measuring between these.
Normal cardiac contours

The left heart contour (red line) consists of the left lateral border of the Left Ventricle (LV).
The right heart contour is the right lateral border of the Right Atrium (RA).
Assessing the heart
- The lingula of the upper lobe of the left lung wraps over the left ventricle, and so the loss of definition of the left heart border may be related to disease in this area of the lung.
- On the right, the middle lobe is located adjacent to the right atrium, and therefore loss of definition of the right heart border may be due to increased density caused by disease in this lung lobe.

Mediastinal contours
- The mediastinum itself contains the heart and great vessels (middle mediastinum) and potential spaces in front of the heart (anterior mediastinum), behind the heart (posterior mediastinum) and above the heart (superior mediastinum). These potential spaces are not defined on a normal chest X-ray, but an awareness of their position can help in describing the location of disease processes.
- There are several structures in the superior mediastinum that should always be checked. These include the aortic knuckle, the aortopulmonary window, and the right para-tracheal stripe.

Normal aortic knuckle
- The aortic knuckle represents the left lateral edge of the aorta as it arches backward over the left main bronchus
- The contour of the descending thoracic aorta can be seen in continuation from the aortic knuckle
- Displacement or loss of definition of these contours can indicate diseases such as aortic aneurysm or adjacent lung consolidation
Normal aortopulmonary window

- The aortopulmonary window is located between the Aortic Knuckle (AK) and the Left Pulmonary Artery (LPA)
- It is a space where abnormal enlargement of mediastinal lymph nodes can be seen on a chest X-ray
Soft tissues
- The soft tissues are often overlooked when viewing a chest X-ray, however, abnormalities of the soft tissue may give important clues to a diagnosis. Whenever you look at a chest X-ray, have a look at the soft tissues, especially around the neck, the thoracic wall, and the breasts.
- If a patient has very thick soft tissue due to obesity, underlying structures such as the lung markings may be obscured. Large breasts may obscure the costophrenic angles, giving the impression of the presence of pleural effusions.
Bones
Clavicles – Spinous processes – Ribs
- The spinous processes of the vertebrae (posterior structures) and the medial ends of the clavicles (anterior structures) are landmarks to assess rotation.
- The ribs should be checked on every chest X-ray.

Clavicle – Scapula – Humerus
- The clavicles, scapulae, and humeri are often clearly seen on a chest X-ray
- Occasionally you will see evidence of important disease such as metastases in these bones

- Clavicle
- Acromioclavicular joint
- Acromion process of scapula
- Body of scapula
- Glenoid fossa of scapula
- Head of left humerus
- Glenohumeral joint
- Coracoid process of scapula
Watch the first part of How to interpret chest X-Ray: Quality
Download Chest X-Ray Anatomy: How to Interpret Chest X-Ray PowerPoint File

{kind=link}